
It’s that time of year — allergy season. The warm weather is here and everything is blossoming. Here are some recommendations for allergy treatments.
First-line treatment for mild seasonal allergies includes oral second-generation antihistamines (cetirizine, fexofenadine, loratadine, levocetirizine, desloratadine) or intranasal antihistamines (azelastine, olopatadine).
Cetirizine, fexofenadine, and loratadine are available over-the-counter: Cetirizine: Zyrtec, Fexofenadine: Allegra, Loratadine: Claritin, Alavert
Intranasal azelastine antihistamines are prescription-only in the United States and are not available over the counter.
For moderate to severe symptoms, intranasal corticosteroids (fluticasone, mometasone, budesonide, triamcinolone) are the most effectivemonotherapy. [1-3]
All four intranasal corticosteroids are now available over-the-counter (OTC) — they include Flonase, Nasonex, Rhinocort, and Nasacort.
The following table outlines the stepwise approach to treatment based on symptom severity:
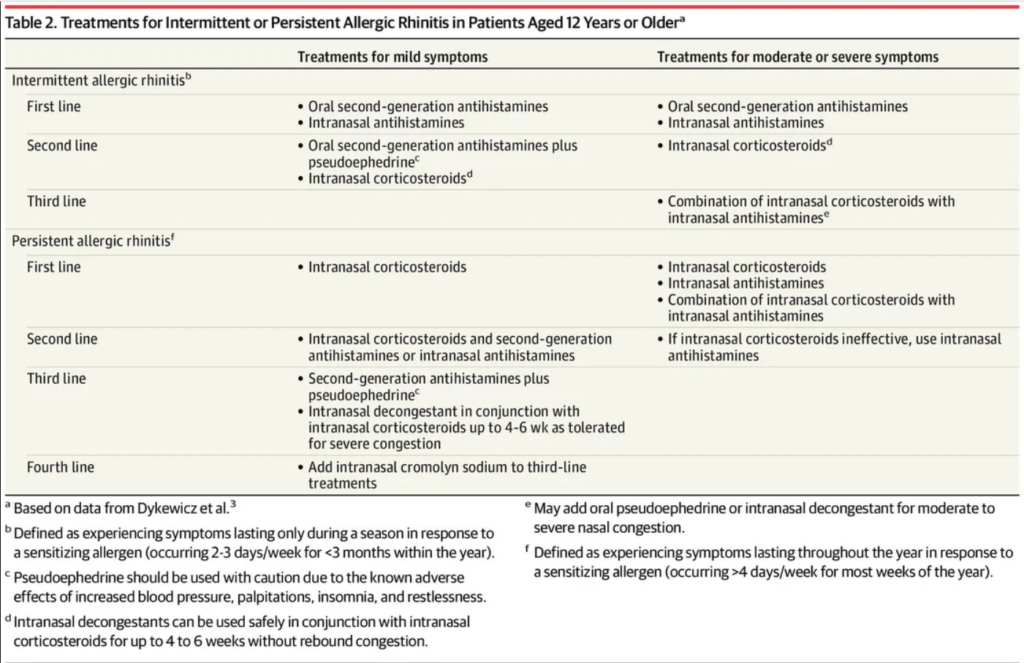
Mild intermittent symptoms: Oral second-generation antihistamines or intranasal antihistamines are appropriate first-line options. These medications have rapid onset and can be used on an as-needed basis. Many are available over the counter, including loratadine, cetirizine, and levocetirizine. [1]
Moderate to severe symptoms: Intranasal corticosteroids are considered the most effective pharmacotherapy for seasonal allergic rhinitis and are recommended as first-line topical monotherapy by most consensus guidelines. [1][3] The 2017 Joint Task Force on Practice Parameters strongly recommends intranasal corticosteroid monotherapy over combination therapy with oral antihistamines for initial treatment. [2] Clinical effects appear within a day, though peak effect may take several weeks. [3]
Combination therapy: For moderate to severe seasonal allergic rhinitis, the combination of an intranasal corticosteroid and intranasal antihistamine may be considered for initial treatment. [2] This approach can be more effective than monotherapy in patients with persistent or severe symptoms. [1]
Additional considerations: Saline nasal irrigation may reduce symptom severity and is relatively inexpensive. [1] Oral decongestants (pseudoephedrine) can be added for severe congestion but should be used with caution due to cardiovascular side effects. [1] Topical nasal decongestants should only be used short-term (up to 4-6 weeks) to avoid rebound congestion. [1][3] Leukotriene receptor antagonists like montelukast are less preferred than intranasal corticosteroids and carry a boxed warning for neuropsychiatric effects. [1-2]
Severe exacerbations: A short course of oral corticosteroids (35-40 mg for 5-7 days) may be appropriate for severe acute exacerbations, but intramuscular corticosteroids are not recommended. [1]
If you need some further guidance or do not respond to over-the-counter remedies, then please reach out to our office at (707) 938-1255 to schedule a visit.